2025 – PAGE 84 – ENDOCRINOLOGY
21-HYDROXYLASE DEFICIENCY RELATED CONGENITAL ADRENAL HYPERPLASIA
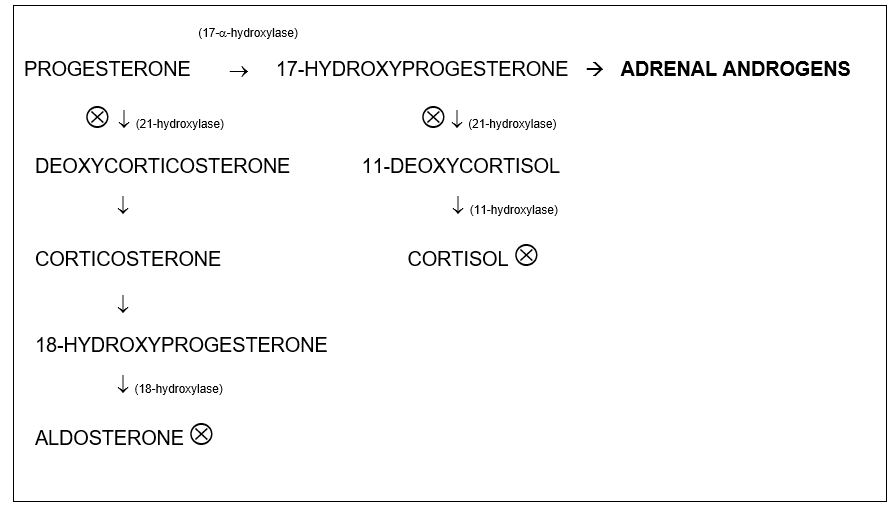
11-HYDROXYLASE DEFICIENCY
11-HYDROXYLASE DEFICIENCY can also cause Congenital Adrenal Hyperplasia, but is much less common. This is probably not the answer that the ABP is looking for, but be familiar with it. If a patient has symptoms/labs consistent with Congenital Adrenal Hyperplasia and also has hypertension, then this is the answer. This is a non-salt wasting form of CAH, so sodium levels are NORMAL.
MNEMONIC: 11 = 1–1 = H = HTN. The 11- in 11-Hydroxylase Deficiency can be made to look like the H of HTN, or “1–1TN.” It works even better on paper. Try it!
17-HYDROXYLASE DEFICIENCY
17-Hydroxylase deficiency is an extremely rare cause of Congenital Adrenal Hyperplasia. There is decreased cortisol and sex steroid synthesis, and increased mineralocorticoid synthesis. This results in Congenital Adrenal Hyperplasia symptoms + HYPERTENSION + hypokalemia. You can also have a metabolic alkalosis.
PANHYPOPITUITARISM
In panhypopituitarism, low ACTH levels result in decreased production of androgens, so this CAN present with ambiguous genitalia and/or a micropenis in males. It WILL be accompanied by hypoglycemia because of decreased cortisol production.
AMBIGUOUS GENITALIA & DISORDERS OF SEX DEVELOPMENT (DSD)
NOTE: This section is ripe for questions on the smallest nuances. If you understand a few key points, you’ll sail through these questions. Most review books simply give you the name of a disease and the associated findings for this section. Understanding the PEARLS below will be instrumental in helping you understand these conditions.
| Sex chromosomes DSD | 46,XY DSD | 46,XX DSD |
| 45,X (Turner syndrome) | Disorder of gonadal (testicular) development: complete/partial gonadal dysgenesis | Disorder of gonadal (ovarian) development: complete/partial gonadal dysgenesis |
| 47,XXY (Klinefelter syndrome) | Disorder in androgen synthesis or action: e.g. androgen insensitivity syndrome | Extragonadal androgen excess: e.g. congenital adrenal hyperplasia |
| 45,X/46,XY or 46,XX/46,XY | Others: severe hypospadias | Others: vaginal agenesis |
PEARLS:
- The default structure/phenotype of all embryos is the FEMALE phenotype (hence, it’s an EASY and PASSIVE process), including the creation of Mullerian Ducts. Those need to REGRESS to give a male INTERNAL phenotype.
- For embryos with a Y chromosome, the PRESENCE OF ANDROGENS and FUNCTIONAL RECEPTORS create the male EXTERNAL genitalia. BOTH must be present. So if there are no androgens, a penis and scrotum are not created from the default vagina-like structure.
- The “Y” chromosome also means the embryo should produce the MULLERIAN INHIBITOR HORMONE/ FACTOR/SUBSTANCE (MIH/MIF/MIS), which results in the regression of the default FEMALE INTERNAL duct structures.
MNEMONIC: Sorry ladies, but for the sake of this mnemonic, just go with the idea that women are passive/easy. “Becoming a woman is PASSIVE/EASY. Becoming a MAN is HARD!” HARD → MAN. I think you get the picture.