2025 – PAGE 262 – 263 – GENETICS & INHERITED DISEASES
TRISOMY DISORDERS
PEARLS: The risk of ALL trisomy disorders increases with maternal age. Women who are 35 years of age and older are considered at high risk. There is an increased risk of having a VSD, especially with Trisomy 21. Know that Trisomy 21 is referred to as Down Syndrome, but you are not likely to be asked to recognize that Trisomy 18 is Edwards Syndrome, or that Trisomy 13 is Patau Syndrome.
DOWN SYNDROME (AKA DOWN’S SYNDROME)
The term Down Syndrome (AKA Down’s Syndrome) specifically refers to having three Chromosome #21s but does NOT differentiate between someone having a TRISOMY 21 Down’s (due to a nondisjunction during gametogenesis) versus a Translocation Down’s. Down Syndrome is the most common cause of intellectual disability. Fragile X is the most common inherited cause of intellectual disability.
- CLASSIC FINDINGS include a rounded face, almond-shaped eyes with upslanting palpebral fissures, flat nasal bridge, macroglossia, a single transverse palmar crease (AKA “simian crease”), poor muscle tone (hypotonia), and a wide space between the first and second toes (AKA “sandal toe”).
- OTHER POSSIBLE FINDINGS
The patient may also present with AV canal defect, VSD (AV canal >> VSD), atlantoaxial instability, small phallus (similar to Prader Willi), excess nuchal skin, clinodactyly (incurved pinkie finger), obstructive sleep apnea with right-sided heart failure, and mild intellectual disability. Patients can usually live independently. Males are typically infertile, while females are not. All patients have an increased risk of leukemia.
-
- IMAGE: (Brushfield Spots) www.pbrlinks.com/DOWNSYNDROME3
- PEARL: Knowing the etiology of a patient’s Down’s is extremely important for the purposes of counseling. Since this is such a confusing topic, if all else fails, just choose to do a karyotype on the baby or the parents and MOVE ON TO THE NEXT QUESTION.
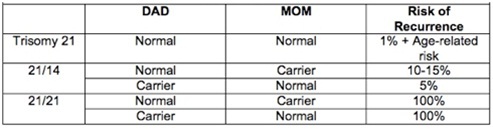
- TRISOMY 21 DOWN’S: This is the most common form (95%) and is due to nondisjunction of chromosome 21. A karyotype of Mom and Dad’s chromosomes is NOT needed because they would show normal chromosomes. The risk for recurrence of TRISOMY DOWN’S in future pregnancies is equal to the mother’s age-related risk plus 1%.
- TRANSLOCATION DOWN’S: This is very confusing. Parental karyotyping IS needed. Please start by looking at the shortcut below. If that is enough for you, MOVE ON. Essentially, if the child’s karyotype shows a translocation, get karyotyping of both parents’ chromosomes. The carrier parent will have either the main part of chromosome 21 attached to a different numbered chromosome (usually chromosome 14, in which case this is a partial translocation), or the main part of one chromosome 21 will be attached to the main part of another chromosome 21. The second possibility may be shown as t(21q;21q) and carries a 100% risk of future Translocation Down Syndrome babies because that parent only has that chromosome (21 attached to 21) to donate. The first possibility (in which 21 is attached to 14) carries about a 10-15% chance of future Down’s pregnancies if the MOM is the carrier, and about a 5% if the DAD is the carrier. If you take the time to work out the actual inheritance pattern, it’s theoretically 33%. But nature doesn’t seem to care. In any translocation carrier, that person’s siblings should also be given the opportunity to be screened.
- SHORTCUT:
Trisomy 21: Age related risk + 1% is the risk of future Down’s pregnancies.
Translocation in which the parent is carrying a 21 attached to 21: 100% risk (all future children will have Down’s).
Anything else: < 15% Risk
LINK: www.pbrlinks.com/DOWNSYNDROME4
SUMMARY TABLE:
- DOWN SYNDROME HEALTH SUPERVISION
Children with Down syndrome often have, or acquire, multiple health issues that can include vision problems, thyroid disease, diabetes, celiac disease, seizures, heart disease, hearing loss, sleep apnea, hematologic disease, atlantoaxial instability, and others. Keep an eye out for anything in the history of a Down Syndrome child that might warrant further workup in a question asking you about the best “next step” in management.
- ATLANTOAXIAL INSTABILITY IN DOWN SYNDROME
Suspect this in any Down syndrome patient with a history of a gait disturbance or any other neurologic signs. Reflexes may be brisk. There is no role for routine screening with X-rays in asymptomatic Down Syndrome patients. This diagnosis can be a tricky to make because there is atlantoaxial INSTABILITY between C1 and C2, so the X-ray findings can change over time from normal to abnormal and vice versa. Therefore, if you suspect the diagnosis, don’t be shy about repeating an X-ray, or even getting an MRI (required if there are clear symptoms).