2025 – PAGE 132 – CARDIOLOGY
TETRALOGY OF FALLOT (TOF)
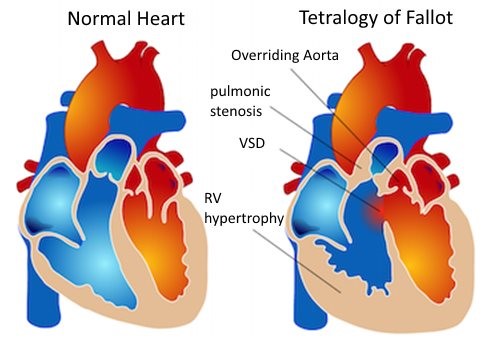
Tetralogy of Fallot is the most common cardiac cause for cyanosis in children (of any age). The four primary findings include PULMONARY STENOSIS (PS), RVH, OVERRIDING AORTA, and a VSD. The EKG shows RAD consistent with RVH. The exam reveals a PS murmur (harsh LUSB murmur, a single s2, a single S1, and possibly a click). Note that the P2 component is SO soft that it simply sounds like a single S2. There is a RIGHT to LEFT shunt at the VSD because blood cannot flow to the lungs due to the PS. Therefore there is NO pulmonary hypertension or evidence of congestion on the CXR (look for a clear CXR). That also means giving PGE will result in a PDA shunting blood from the LEFT to the RIGHT (from the Aorta to the PA, with no concerns for directional change from pulmonary hypertension). CXR findings include a lack of vascular congestion, a BOOT shaped heart, and RVH.
- MNEMONIC: “You have to PROVe it is a TET!” = PS, RVH, Overriding aorta, VSD!
- TET SPELLS: Episodes of cyanosis (the precise mechanism is uncertain) possibly occurring at times of relative anemia or increased pulmonary vascular resistance. An acute increase in Right to LEFT shunting occurs, which results in cyanosis, possible syncope, or even death. Older children squat, younger children’s knees are forced to the chest in order to increase systemic vascular resistance and decrease/reverse the flow of the shunt. Other possible treatments include morphine, phenylephrine, propranolol, and volume.